
(This column first appeared in Broad + Liberty)
The controversy over the treatment of transgender children has reached explosive heights and is often weaponized in political circles. Throughout this debate, it has been difficult to express concern and support for these kids in distress without being labeled transphobic. I recognize the pain of these young people and also have major concerns about medical interventions before the age of eighteen.
The two positions are not mutually exclusive, despite what you may have read in the mainstream media.
“Do you want a dead daughter or a living son?” This is the rationale often given to parents whose child is experiencing gender dysphoria or gender incongruence.
Under the tenets of “gender-affirming” care, some mental health professionals and physicians advise parents that they should allow their child to transition to a different gender lest they commit suicide.
According to the American Academy of Pediatrics, “Gender-affirming care reflects a range of interventions meant to support an individual when their gender identity conflicts with the one assigned to them at birth. Until the patient is eighteen years of age, gender-affirming care generally refers to developmentally appropriate support as the child goes through a social transition (eg, changes in pronouns, names, hairstyles, and/or clothing), puberty blocking treatment, and/or hormone replacement therapy (HRT).”
Locally and across much of the United States, gender-affirming care is the standard for treating children with gender incongruence/dysphoria, despite the fact that there is very little research to support this model.
Earlier this month, an independent review of gender identity services for children and young people — known as the Cass Review after its lead author, Hilary Cass — was published in Britain. The review is groundbreaking and may revolutionize the treatment for children and adolescents. It has already changed policies and practices in multiple European countries.
The review is comprehensive and thorough, citing numerous research studies across the globe, while at the same time honoring the voices of children, young people, and their families who are struggling with these issues. The 350-page report demonstrates a scholarly research methodology and also a compassionate approach for those seeking treatment and support. The review is accessible to not only clinicians and physicians, but also to lay people. The author went to great lengths to weave in the “lived experiences” of young people who are often desperately seeking medical treatment.
Within this framework, Cass, a retired pediatrician, laid out numerous recommendations and changes to the current UK health system for transgender youth.
Key findings include:
- Due to the lack of evidence and potential side effects, puberty blockers and hormones should not be given to children unless they are in a clinical trial. These drugs in children may impact bone density, executive functioning, height, weight, psychological functioning, and metabolic health. (#101, p. 34)
- It is important for parents to be involved in their child’s treatment.(#10.53, #10.57, p. 143)
- There is an exponential increase in young women experiencing gender dysphoria/incongruence. (#5.69, p. 97)
- A high percentage of transgender youth have co-occurring mental health issues, in addition to a high number of youth on the autistic spectrum. Many youth seeking treatment have experienced significant adverse childhood events, including trauma. (#5.26, p. 91 – #5.36, p. 92 – #5.48, p. 94)
- There is no evidence to support that suicide decreases with transition or hormones. (#86, p. 33)
While I sincerely hope that the US will adopt some of these recommendations from the review, there are local organizations that could benefit from reading this report and potentially change policies based on the findings.
Implications for Pediatric Medical Practices
Children’s Hospital of Philadelphia (CHOP) is the largest local provider of pediatric services to children. Their Gender and Sexuality Development Clinic “offers psychosocial and medical support for gender variant, gender expansive, and transgender children and youth up to age 21 and their families.”
According to their website, the clinic is experiencing rapid growth. “While we typically have averaged between 250 to 350 new families in a year, we welcomed more than 800 new families to our Gender & Sexuality Development Program in 2021.” (The 2021 update is the most recent listed on their website. A request for the last five years of annual reports was not returned.)
In 2020, clinic co-founder Nadia Dowshen testified to the Pennsylvania House of Representatives Subcommittee on Health Care, assuring legislators that these medical interventions are reversible and safe. Some of her testimony is refuted in the newest review.
“The major medical intervention that is considered fully reversible is puberty blocking medication. These medications are only given when a child has already started puberty, which can be distressing to youth with gender dysphoria, and has displayed insistence, consistence and persistence in their gender identity. Again, these decisions are made together by the care team, youth and parents. This is a very safe medication that had been used for many decades previously for children who are starting puberty too early or what is referred to as precocious puberty.”
The review states that puberty blockers were only approved for use for precocious or early puberty, not for adolescents in the midst of puberty and there is not enough evidence to determine whether there are side effects or long-term, irreversible consequences for this population. Dowhen further testifies that these drugs help to prevent suicide for transgender youth, and the review refutes that assertion as well.
“It has been suggested that hormone treatment reduces the elevated risk of death by suicide in this population, but the evidence found did not support this conclusion.” (#86, p. 33)
I requested comments four separate times from CHOP and the clinic co-founders regarding their thoughts about the review, the clinic’s annual budget, the number of gender reassignment surgeries performed, and the percentage of patients prescribed puberty blockers or hormones. None of the requests were returned with the exception of an out-of-office automatic response from Dr. Dowshen.
The only information that I have been able to obtain about the costs of procedures and medications comes from a Right to Know Request submitted by PA Family. The state of Pennsylvania fulfilled the request and provided the following information regarding Medicaid funds expended for these services.
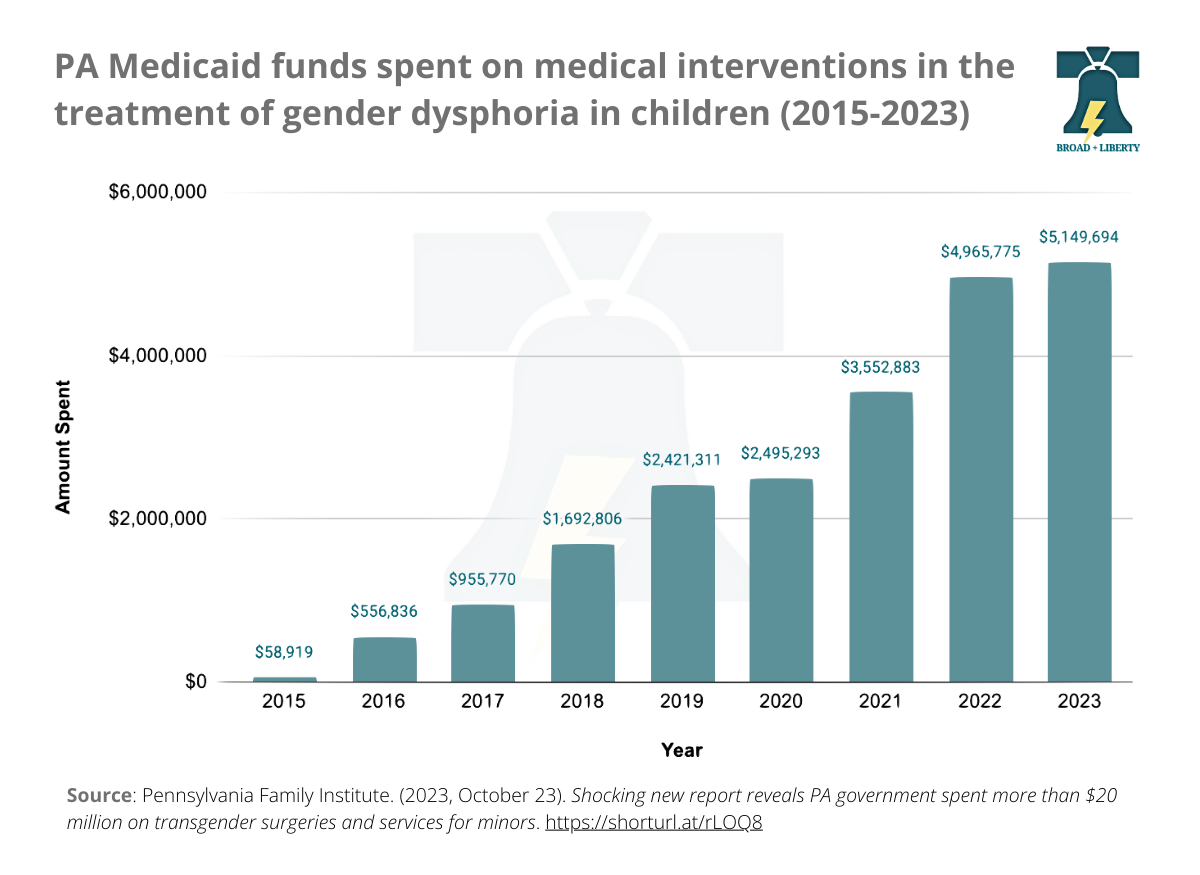
According to the notes from the state, the data was limited to recipients aged 18 and under. “This file provides information on Pennsylvania Medical Assistance spending on sex reassignment and transition related services and drugs for service dates between January 1, 2015 to December 31, 2023.”
The chart clearly shows that medical interventions (puberty blockers, hormones, and medical procedures) utilized in the treatment of gender dysphoria/incongruence and paid for by the state — which is to say, by the taxpayers — has increased exponentially since 2015 with over $5 million spent last year alone.
In light of the current review, the state should consider suspending the approval for these services unless the recipients are enrolled in a clinical trial. CHOP should also consider halting medical treatments absent a clinical trial and should be more forthcoming with their aggregated data.
CHOP is not the only local pediatric practice that provides medical interventions in the treatment of gender dysphoria/incongruence. Nemours Children’s Health has a “gender wellness program” that can include the prescription of puberty blockers and hormones.
Implications for School Districts
In the local region, many school districts have adopted policies related to transgender students. While many of the policies are likely well-intentioned to protect transgender youth against bullying and other issues, they also contain statements about keeping information from parents. For example, Great Valley School District in Chester County has Policy 103.3, Transgender and Gender Expansive Student, that includes this statement:
“All persons, including students, have a right to privacy, which includes the right to keep private one’s transgender status or gender expansive presentation at school. Therefore, school personnel should not disclose information that may reveal a student’s transgender status or gender expansive presentation to others, including the student’s parents/guardians and/or other school personnel, unless legally required to do so or unless the student has authorized such disclosure.” (emphasis added)
A quick sampling survey shows that other districts have adopted similar language, including Radnor and Haverford in Delaware County, Wissahickon in Montgomery County, and New Hope-Solesbury in Bucks County.
Throughout the review, the words “parent” and “carer” are used almost 200 times. The report clearly states that parental involvement and support for parents are important throughout the process of care for young people experiencing gender dysphoria/incongruence.
Despite their best intentions, these policies may do more harm than good in terms of supporting children who are experiencing gender dysphoria/incongruence. Parents must be involved and informed if their child wants to be called a different name or pronoun. Given the high rate of co-occurring mental health issues for this population, secrecy from parents is not appropriate and may border on unethical. Most school districts do not have the capacity to address significant mental health issues, and even if they do, treatment should only be done in collaboration with parents to ensure the best possible outcomes for the child.
Next Steps
The Cass Review has local and national implications regarding the best practice of care for children dealing with gender dysphoria. It presents an opportunity for local pediatric medical practices and school districts to evaluate their policies and practices to determine if they are aligned with the new findings.
Physicians take an oath to do no harm, and school district staff and administrators have an ethical responsibility to protect young people from harm. If we are truly committed to supporting and helping children suffering from gender dysphoria, then we have a moral obligation to re-evaluate our current practices.
While some may be upset with initial changes in policy and protocols, we must be concerned about the long-term consequences of these decisions. We must address the entire child, especially other mental health issues. As adults and decision-makers, it is our responsibility to protect these young people.
The bottom line is that we simply do not have enough information nor research to support the current practice of prescribing puberty blockers or hormones to children. Absent a robust clinical trial, local pediatric facilities should discontinue this practice and Medicaid should stop paying for it.
Standing up for children and following science even when it is unpopular should not be political. Both sides of the debate have weaponized this vulnerable population to advance their own agendas. It is now time to simply do what is right and follow the recommendations in the Cass Review to ensure the best possible outcomes for these young people.
